How DMSO Protects and Heals the Internal Organs
The evidence behind DMSO's utility for a myriad of challenging diseases

Story at a Glance:
•The therapeutic actions of DMSO make it well suited to treat challenging conditions throughout the body, including many of the internal organs.
•In this article, we will examine how DMSO protects organs from injury (e.g., poisoning or blood loss) and some of the specific diseases DMSO has been proven to treat.
•These include: heart attacks, liver cirrhosis, gallstones, ARDS, lung damage from inhaling smoke, pulmonary fibrosis, pancreatitis, diabetes, nephritis, kidney stones, polycystic kidney disease, cystitis, epididymitis, genital pain, prostatitis, urethral syndrome, enlarged prostates, tubal infertility, endometrial inflammation, and fibrosis.
•This article will review DMSO treatment protocols for those conditions (along with non-DMSO approaches we utilize for them) and provide general DMSO information for those looking to use DMSO for their own health.
Note: when this article was emailed out, the research in the section “Kidney Function” was accidentally replaced with another part. This has been fixed.
Dimethyl sulfoxide (DMSO) is a remarkably safe compound that can treat a variety of challenging conditions. Since DMSO is remarkably effective for treating chronic pain, arthritis, and injuries like sprains or burns (discussed further here), it quickly spread across America as a miracle drug. Thousands of studies were conducted to confirm its value, and before long, hundreds of thousands of people considered it to be the most important therapeutic ever discovered.
Unfortunately, due to various negative political factors, the FDA went from embracing DMSO to going to war against it, and eventually, the pharmaceutical industry reluctantly followed suit. Sadder still, the FDA refused to relent even once:
•DMSO was shown to effectively treat strokes, traumatic brain injuries, spinal cord injuries, and many circulatory disorders (discussed here).
•DMSO was shown to cure a variety of “incurable” autoimmune and connective tissue disorders (discussed here).
•DMSO was shown to treat a variety of challenging (and often incurable) eye, ear, sinus, and dental conditions such as tinnitus and blindness (discussed here).
Since publishing those articles, I’ve received roughly a thousand reports from people of the remarkable effects DMSO has had on them (which can be read here), which while unbelievable, are almost identical to what people experienced in the 1960s before the FDA erased DMSO from the public’s memory.
Likewise, I’ve received almost as many questions (which is why I am trying to make these articles as thorough as possible). One of the most common questions I’ve received is if DMSO can help with various disorders of the internal organs. After realizing I did not have enough data to answer some of them within my drafts for this series, I spent a few weeks going through search engines combining each permutation of DMSO (e.g., dimethylsulfoxide) and each organ or the common diseases of them so I could identify the pertinent studies to share here. Despite my best efforts, I likely missed some, so if you are aware of any that should be added, please send them my way.
As you review these studies, you will notice a few patterns.
First, many were animal studies (something that always makes me sad), which used research protocols existing at the time to induce common diseases and then see if DMSO could prevent them. For example, cutting off the blood supply to tissues in the body will injure them, particularly when the blood flow comes back, so this can be modeled by clamping an artery that feeds the organ (typically for around an hour) and then unclamping it, creating what is known as an ischemia-reperfusion injury.
Second, DMSO has many benefits for other parts of the body (e.g., reducing autoimmunity, increasing blood circulation, and healing injured tissues). One disease process (which I haven’t discussed for over a year) is particularly important to understand since, like poor circulation, it underlies many illnesses:

There are a few key points about this model:
•Typically, more potent stressors make it progress faster (e.g., strokes rapidly kill brain cells). In contrast, weaker and more chronic stressors make it progress slower (e.g., I previously discussed how the cell danger response underlies many “inexplicable” chronic diseases).
•The further down this progression a tissue is, the harder it is to reverse (but with the correct therapy it can almost always be done).
•Many regenerative therapies essentially work by getting “shocked” cells to come back to life and start working again, which in many cases is critical for overall health since those tissues not working can disrupt the entire body.
•DMSO can reverse this process (discussed further in the first part of this series), but it is typically more helpful for the rapidly progressing instances coming from a significant stressor (e.g., a stroke or a severe injury or ingesting a poison). This in turn, explains why DMSO can sometimes give motor function back to people who were paralyzed by strokes years ago, but it is dramatically more effective if given shortly after a stroke, traumatic head impact or spinal cord injury, and likewise why individuals on DMSO suddenly “notice” things in their body that had stopped working come back.
•For slower and more chronic versions of this process which have already progressed, one typically needs a systemic regenerative therapy (discussed further here).
Let’s now look at what DMSO does for each organ.
Heart
Most of the studies discussing DMSO’s interactions with the heart regard its ability to protect it from permanent ischemia-reperfusion injuries (e.g., heart attacks):
•In a 2012 study, rat hearts had their blood supply cut off for 30 minutes and then were reperfused for 120 minutes. DMSO being given beforehand was found to reduce the resulting tissue necrosis (death) significantly and left ventricular dysfunction, particularly if it was given for a few days beforehand, rather than just immediately preceding the blood supply being cut off. Similar results were reported in 2010 and in 1981 when a heart attack was simulated. Additionally, a 1987 study found that DMSO increased the heart’s cardiac output during a heart attack (and how much blood was able to get to the brain).
•A rabbit study found that if hydrogen peroxide (H₂O₂) was given concurrently with DMSO immediately after cutting off the blood supply to the heart, the damage the heart experienced was further reduced, presumably due to H₂O₂ providing oxygen to the heart tissue.
•When ischemic hearts are reperfused with a calcium ion containing solution, significant damage occurs. A rat study found that if DMSO was given in conjunction with the calcium solution, that damage was significantly reduced. A related rat study found DMSO prevented ischemia-reperfusion injuries from causing severe contractures in heart cells and the formation of contraction bands, and that this seemed to be linked to DMSO reducing the oxygen induced creatine kinase release from cells.
•One mechanism to explain the damage that occurs in heart cells after a shock or stressful conditions (e.g., heart failure) is that the t-tubules within the heart cells will seal and remodel. In one study, 1% DMSO (but not 10% DMSO) was found to prevent this from occurring and this process was hence hypothesized to at least in part explain DMSO’s ability to protect heart cells from significant stressors.
Additionally:
•Isoproterenol can cause heart damage similar to that seen after a heart attack. Giving rats DMSO after giving the isoproterenol was found to reduce the resulting myocardial fiber necrosis, prevent ventricular aneurysms and cardiac rupture, and result in a smaller residual area of myocardial fibrosis.
•A key component of regenerative medicine is using stem cells (which have the potential to differentiate into many different cells) to replace damaged tissues (particularly those within critical organs). DMSO (especially with another medication) was shown to cause stem cells to differentiate into heart cells.
•When heart cells were exposed to low concentrations of DMSO (less than 0.5%), their respiratory control ratio and cellular viability relative to the control cells were enhanced (whereas at 3.7%, DMSO became harmful to them).
•DMSO was found to prevent heart damage caused by dietary copper deficiency.
•DMSO can also increase or decrease the force of heart contractions (e.g., a 70 mM DMSO concentration or less has a positive inotropic effect, while a higher one can do the opposite or create a mild hyperpolarization that prolongs the action potential) in a manner independent of beta-adrenergic receptors, and does not alter cardiac rhythm.
Intestines and Stomach
Most of the research I know that has been done in the gastrointestinal tract was for using DMSO to heal irritation, inflammation, and bleeding of the gastrointestinal tract (with the only exception I know of being a study that showed DMSO increased the stomach’s sensitivity to vagal stimulation).
For example, in a previous article, I mentioned that my colleagues use DMSO for irritable bowel syndrome and cited a 1968 patent that stated DMSO had helped a significant number of people with acute or chronic gastritis, peptic ulcers, enterocolitis, and mucomembranous colitis). The other gastrointestinal studies are as follows:
•A double-blind, randomized study evaluated patients with recurrent attacks of proctosigmoidal ulcerative colitis that were not being prevented by their prophylactic medical regimen, three different combinations of standard therapies, or a standard therapy with DMSO (46) or allopurinol (45). After two weeks, 51% recovered from a standard regimen (sulfasalazine or prednisolone), while 84% of those using DMSO or allopurinol recovered. Over the next year, those treatments were continued and it was observed that the standard treatment (sulfasalazine) had a 25% relapse rate, whereas that rate was only 5% of those taking DMSO or allopurinol.
•A study evaluated hospitalized patients with pelvic fractures or hypovolemic shock who were at risk for a stress induced gastric ulcer. Of the 58 controls, 22% developed one, whereas of the 57 receiving DMSO, only 4% did (along with 3% of 62 who received allopurinol). Additionally, none of those receiving DMSO deteriorated or required emergency surgery, whereas 8 controls and 1 allopurinol recipient did (of whom 3 then died).
•A study randomized 302 consecutive patients with previous symptomatic duodenal ulceration that was shown to have healed, and who were smokers and social drinkers, to receive four different treatments. Of the 220 available for evaluation, 65% who received a placebo had a recurrence of the ulcer, 30% of those who received cimetidine, 12% of those who received allopurinol, and 13% of those who received oral DMSO.
•A randomized double-blind study of 363 consecutive patients whose duodenal ulcers that did not heal despite 3 months of treatment with cimetidine (and who were cigarette smokers or social drinkers), were given either cimetidine twice a day alone or with DMSO or allopurinol. In 315 patients who were evaluable for analysis, at 8 weeks, 60% of those who had cimetidine recovered, whereas 100% of those who received DMSO or allopurinol recovered. Additionally, the one year relapse rate was 29% for cimetidine alone, 8% for those who took allopurinol, and 7% in those who took DMSO.
•A randomized double-blind study took 238 patients with symptomatic acute duodenal ulceration who were smokers and social drinkers were randomized to receive for 8 weeks cimetidine or 8 weeks of a half dose of cimetidine plus oral DMSO (400mg two times a day) or allopurinol. After 8 weeks, 69 of the 87 (79%) who only received cimetidine recovered, whereas all of the 85 who received DMSO and 84 who received allopurinol did. Additionally, 67% of those who received cimetidine over the next year relapsed, compared to 6% of those who took DMSO and 5% of those who took allopurinol.
•A randomized study took 101 patients presenting with hematemesis (coughing up blood) due to erosive gastritis (a fairly dangerous condition). It gave them either saline or oral allopurinol and DMSO orally every 6 hours for 5 days. Of the 50 controls and 48 who were treated (along with 2 who left because they could not tolerate the treatment), 29% of the controls and 8% of who were treated had further episodes of hematemesis (with three of the controls requiring subsequent surgery—one of whom died). Of those who remained stable, a subsequent endoscopy showed evidence of hemorrhagic inflammation in 44% of controls and 9% of those who received DMSO and allopurinol.
Note: the six previously listed studies were conducted in Iraq between 1990-1994. What many don’t know is that prior to the harsh economic sanctions on Iraq and subsequent bombing campaigns, the country was regionally recognized for its robust medical system (which then collapsed), a situation almost identical to what happened to Libya’s healthcare system after NATO toppled its government.
•Another author reported on a doctor who had 5 patients with recurrent duodenal ulcers and were social drinkers he gave DMSO to. They were examined once a month for a year, and all 5 had no recurrence of ulcer symptoms (along with having better health than expected and excellent attendance at work). He also highlighted the case of a 55 year old woman with severe digestive tract issues (e.g., internal bleeding leading to her being anemic with a hemoglobin of 5.0), weakness, fainting and shortness of breath. After receiving an emergent blood transfusion and being diagnosed with angiodysplasia in her GI tract, she was started on IV iron (which is not pleasant and did not help her causing her to progress to being terminal). She was then started on injected DMSO and B-12, recovered, and over the six years of follow-up, did not require any subsequent blood transfusions.
Note: this type of chronic internal bleeding is quite challenging to treat (e.g., the only other approach I know of that consistently helps here is a Chinese herbal formula).
•Cutting off the blood supply to the small intestine will rapidly cause the tissue there to die and often rupture (leading to fatal peritonitis). In rats, giving IV DMSO to rats after 30-60 minutes of the intestinal blood supply being cut off, resulted in 28 out of 29 not developing gangrene, and within 24 hours, there was no evidence of ischemic damage to the intestines.
Liver and Gallbladder
Many different facets of DMSO’s interactions with the liver, gallbladder, and biliary system have also been researched:
Liver Injury
•A rabbit study, found that DMSO reduced ischemia-reperfusion injuries to the liver that resulted from clamping its artery.
•A rabbit study found DMSO reduced the injury to the liver that resulted from clamping its portal vein.
•In rats, drinking 2 mL/kg of DMSO daily for 4 weeks was seen to prevent dimethylnitrosamine induced liver damage without any major side effects. Specifically, it prevented body and liver weight loss and the induction of hepatic fibrosis and the expression of mRNA for type-1 collagen in the liver. Additionally, DMSO was also found to inhibit LPS induced TNF-alpha and nitric oxide production (e.g., TNF-alpha mRNA levels were reduced).
•A rat study found DMSO inhibited liver necrosis and oxidative stress triggered by injecting D-Galactosamine and restored liver vitamin C levels.
•A rabbit study found that DMSO and tocopherol prevented the liver damage caused by injecting carbon tetrachloride.
•A Brazilian study found that DMSO reduced the oxidative stress that followed part of the liver being surgically removed.
•A study found giving DMSO to rats 10 hours after they were exposed to halothane (an inhaled anesthetic that was phased out of the richer nations due to its toxicity profile), chloroform, or bromobenzene and was found to prevent liver damage these toxicants typically cause. Additionally, they also found DMSO prevented chloroform’s kidney toxicity (renal tubular necrosis) and that none of these benefits resulted when DMSO’s metabolite dimethyl sulfide was given instead. A followup study instead gave DMSO 24 hours later found DMSO reduced the resulting liver damage 4-fold (which without treatment within 48 hours would have occupied 40-50% of the liver) and ALT levels 8-16 fold.
Liver Failure
•This author reported on a study with 12 patients who had terminal liver cirrhosis who agreed to stop drinking all alcohol for the duration of the program were put on daily oral DMSO and aloe vera. Of the 8 who chose to continue the program for 6 months, all had improved health, significantly reduced vomiting, and improved liver function tests, and rather than all being dead within one year as expected, they were in better condition than they had been at the start of the study.
Note: if using DMSO for cirrhosis, it is critical to stop consuming alcohol, as DMSO can slow the metabolism of alcohol.
Gallstones and Jaundice:
•A rat study created obstructive jaundice by ligating (cutting off) the common bile ducts and found that DMSO mitigated the pathologic effects of this (e.g., it normalized laboratory values).
•A Japanese study found that injecting 90% DMSO mixed with 5% hexametaphosphate into the biliary tract effectively dissolved gallstones within the liver and was safe for the patients.
•One study injected DMSO directly into the biliary tree of mice (as sludging of bile in this region can lead to challenging gallstones). That study found that 50% DMSO caused no irritation, but 65% did (e.g., liver enzymes were elevated and necrosis, inflammation and fibrosis were observed). However, the irritation caused by 65% was transient and the rest of the bowel was not affected. Given that direct injections of 50% DMSO caused no issues and typically much lower concentrations of DMSO will contact the bile tract, this suggests DMSO is safe to administer to the biliary tract.
Note: the purpose of this study was to determine if they were harmless agents which could be used to develop treatments for biliary disease (something which can often be quite challenging to deal with).
IV DMSO saved my gallbladder and reduced my inflammation to almost nothing in 2013. Soon after, my alt GI doc no longer had access to it. She was getting it from Switzerland at the time.
Lungs
DMSO protects the lungs from injuries and also helps with a few challenging conditions.
Lung Injuries
•DMSO was found to prevent ischemia-reperfusion injuries to the lungs.
•In rats, DMSO was found to prevent lung injury from hemorrhagic shock (significant blood loss) and transfusing lost fluids back into the circulation.
•Giving DMSO before alloxan (a toxin) was found to prevent the inflammation, cellular damage, and edema alloxan causes in the lungs.
Note: this study also found DMSO prevents acute pulmonary edema.
•DMSO was found to prevent the oxygen deprivation and inability to exchange gasses through the lungs which results from an Ehrlichia ruminantium infection (which is typically fatal).
•In rats, DMSO was found to prevent the significant inflammation and tissue injury which follows a significant traumatic impact to the lung.
•After sheep experienced a lung injury from inhaling smoke, nebulized DMSO (with heparin) was found to reduce the damage to their lungs significantly.
Note: as I have shown in this section, studies exist that show that nebulizing DMSO can be quite beneficial to the lungs. In contrast, a rabbit study found that inhaling 25-50 ml/hr of DMSO for an hour each day for 8 weeks caused pathologic changes in the liver and lungs. While this was a high dose, nebulizing DMSO has nonetheless been advised against in the DMSO field (which I believe was due to that rabbit study). The best conclusion I can draw from these conflicting data points is that DMSO should only be used for acute injuries in the lungs but not chronically nebulized.
Acute Respiratory Distress Syndrome (ARDS)
ARDS is quite challenging to treat (and a common reason people end up on ventilators), so DMSO’s potential to help the condition is quite noteworthy:
•In hamsters, an inflammatory peptide was put into the airway to trigger ARDS (a severe lung condition that often results in ventilation). When DMSO was subsequently given, it was found to reduce the inflammation and fluid in the lungs significantly.
•A similar mouse ARDS study that used bacterial LPS to injure the lungs also found DMSO reduced lung inflammation and fluid leak along with damage to the lining of the lungs.
•A third mouse study found that DMSO prevented LPS damage to the lungs, kept all treated mice from dying (whereas 58% of controls died), and maintained the ability of the lungs to produce ATP.
Note: a few studies have found that DMSO makes a part of the mitochondria able to synthesize ATP (the source of cellular energy) without the rest of the mitochondria being present. This, in turn, hints at the possibility DMSO can allow compromised cells to continue producing ATP (and thereby play a role in preventing cell death).
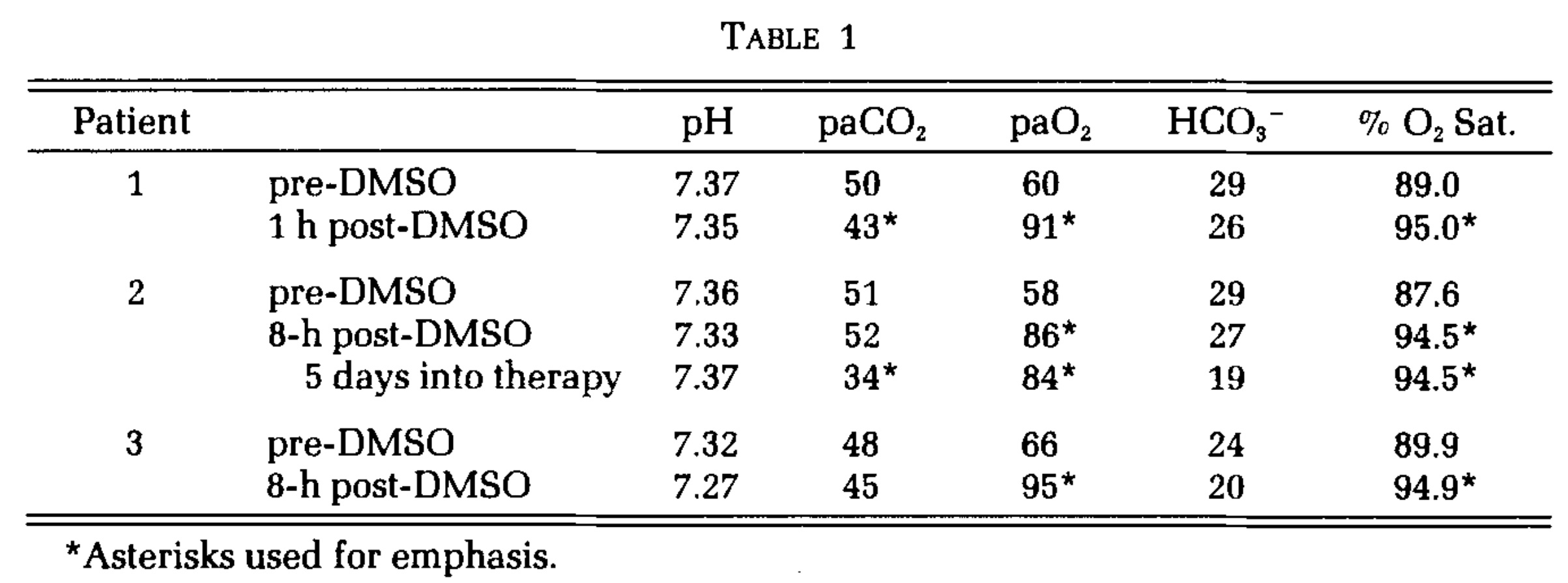
In the one human study where DMSO was used for ARDS (given intravenously at concentrations under 10%) it was found to produce a dramatic improvement in all three patients who received it (e.g., one patient’s lungs were completely normal after a week) and prior to receiving DMSO all three were near death. Additionally, in the one case when DMSO was nebulized, the improvement occurred in 1 hour.
Note: another study found that DMSO reduced immune cell infiltration of a lung infection, which can both be beneficial (as it explains how DMSO prevents the immune system from attacking the lungs), but also problematic as it loses the ability to fight off a significant infection. That study, hence suggests that DMSO should never be used alone as a treatment for bacterial pneumonia (whereas later in this series I will discuss how DMSO can increase the potency of antibiotics).
Chronic Lung Diseases
DMSO was found to reduce chronic pulmonary fibrosis, and this beneficial effect was increased when it was mixed with zinc.
For older patients with chronic respiratory insufficiency (leading to chronically low blood oxygen levels, elevated carbon dioxide levels and an abnormal acid base balance, especially during exercises) due to issues in the lungs or bronchi, daily intramuscular DMSO was found to bring about a recovery without the need for hospitalization in 35/43 (81%).
Note: DMSO has also been shown to treat asthma.
Pancreas
DMSO also shows promise for diabetes and pancreatitis.
Diabetes
Some Type 1 and Type 2 diabetics have reported that DMSO reduces (but does not eliminate) their need for insulin and that DMSO is particularly helpful for the condition since it can also alleviate the pain from diabetic peripheral neuropathy. Studies in this area include:
•Alloxan is toxic to the insulin producing cells of the pancreas and can be used to induce diabetes. A 1977 study found that if DMSO was injected prior to administering alloxan, they did not develop diabetes (although a higher dose of alloxan caused the dose of DMSO only to provide partial protection against diabetes).
•Type 1 diabetes results from the immune system attacking the insulin secreting cells of the pancreas. One strategy for treating type 1 diabetes is to transplant healthy insulin secreting cells into the pancreas. Unfortunately, this strategy often fails because the immune system will attack the transplanted cells too. However, in a mouse study, DMSO was found to protect those transplanted cells by decreasing IFN-γ expression and the number of dendritic, CD8, and Th1 immune cells while increasing Treg cell differentiation—all of which showed DMSO prevents suppresses spontaneous diabetes and autoimmune recurrence of type 1 diabetes.
Note: while type 2 diabetes (the more common form) is not considered to be autoimmune in nature, we have seen many compelling cases suggesting that autoimmunity plays a role in it as well.
•GLP-1 is a key hormone the body uses to regulate satiety and blood sugar (and which diabetes drugs like Ozempic mimic). One study found that 0.5-2.5% DMSO increased GLP-1’s production of insulin by 2-2.5 times. The study’s findings suggest DMSO could help treat diabetes or allow GLP-1 users to use a lower dose of the medication.
•Exposing insulin secreting cells to DMSO was found to enhance glucose-induced and tolbutamide-stimulated insulin secretion without significant effects on basal secretion or potassium responsiveness. Conversely, another study found that at high doses, DMSO would inhibit insulin secretion (however that inhibitory dose is much higher than a DMSO user’s pancreas would ever be exposed to).
Pancreatitis
Another condition, pancreatitis is often quite challenging and dangerous (as there are no conventional treatments for it outside of cases where an obstruction causes it—rather hospitals can only support the patient until they recover). Fortunately, DMSO (and ultraviolet blood irradiation) have been shown to be quite effective for treating it. For example:
•After inducing pancreatitis in rats, DMSO was found to improve pancreatic microcirculation and reduce ICAM-1 expression (a key part of the disease process) and subsequent leukocyte adhesion.
•Another mouse study found DMSO significantly reduced the pancreatic edema resulting from dietary induced pancreatitis.
•A rat study found DMSO protected the pancreas from cerulein induced pancreatitis (e.g., through inhibiting lipid peroxidation in pancreatic tissue, reducing pancreatic edema, reducing how many digestive enyzmes leave the pancreas and reducing the pathologic vacuolization of the pancreas’s acinar cells).
•A randomized double-blind trial took 78 patients with chronic recurring pancreatitis (and no other confounding gastrointestinal disorders) who presented within 2 hours with signs of pancreatitis but did not have signs of generalized peritonitis. Of them, 26 received 10% DMSO rectally, and at least 57% were free of pain after 12 hours (compared to 17% of controls), and all were free of pain after 24 hours (whereas 48% of controls were still in pain). As a result, all DMSO subjects were discharged within 3 days, whereas only 22% of controls were discharged after 5 days of hospitalization.
Note: one German author advocates combining IV DMSO with chlorine dioxide (given at a much slower drop rate) for pancreatitis.
Kidneys
Many different facets of DMSO’s interactions with the kidneys have been researched:
Safety
•A rabbit study found that rabbit kidneys perfused for 60 min with DMSO was unaffected by 1.4M (10.8%) DMSO, but higher concentrations (2.1 and 2.8 M) produced appreciable toxic effects to the kidneys.
A study of paraplegics found that IV DMSO caused no alteration of urinary function or urinary sediment (other than a transient increase in blood cells if osmotic hemolysis occurred from too high of an IV DMSO concentration).
•This study of 7 people found 10-40% IV DMSO caused no acute toxicity to the kidneys.
•A dog study found that in dogs with chronic kidney disease, unless they had stage 4 CKD, DMSO had no adverse effects, and in less severe cases, some improvements were observed.
Note: DMSO often functions as a potent diuretic (although the effects are highly concentration dependent). For example, one dog study found after 1 hour 40% IV DMSO caused a fivefold increase in urination, a rat study found giving it topically five times a day increased urine volume 10-fold, and human study also found 40% IV DMSO caused significant urination. Conversely, this diuretic function is often extremely helpful (e.g., it will take excessive fluid outside of regions it has leaked into) and accounts for some of the significant benefits seen from DMSO.
Ischemia-Reperfusion Injuries
•In a rat study, renal ischemia was induced by cutting off the blood supply to the kidney for 1 hour, after which, DMSO or saline was given intravenously. All the saline treated rats had significantly worsened kidney function and died within seven days, while all the DMSO treated rats survived and had near normal kidney function. A similar experiment was then done in dogs, where DMSO again preserved a near normal kidney function (whereas in the saline treated dogs, 1 died and 4 had transient renal failure).
•Another rat study also found DMSO prevented ischemia-reperfusion injuries.
•A nuclear magnetic resonance imaging study of rat kidneys (a method which makes it possible to detect minute and otherwise invisible changes) found that DMSO protected the kidneys from the damage that occurred when their access to oxygen was cut off, but it did not prevent the transient drop in kidney function which occurred during this period.
Toxic and Dietary Injuries
•A mouse study found if DMSO was given within 3 hours of injecting mercury subcutaneously, it prevented the kidney damage which typically resulted over the next two days (however at 5 hours it was too late). Additionally, the results suggested this protection was not due to DMSO chelating mercury.
•A rat study found DMSO prevented the kidney damage caused by gentamycin, and that (like the previous mouse study) it also restored the levels of GSH and SOD enzyme activity to near normal.
•DMSO was found to protect rats from radiation induced kidney damage.
•In rats with dietary copper deficiencies, DMSO was found to attenuate the increase in blood urea nitrogen and significantly decrease in gamma glutamyl transferase caused by the copper deficiency.
Kidney Function
•When kidney tissues were frozen, DMSO was found to greatly increase the conductivity of the tissue.
•DMSO was found to increase rabbit kidney’s flow rate and changed the GFR, but did not change Na+ reabsorption or fractional water excretion, leading the investigators to conclude DMSO may shift the regulation of urine flow rate from tubular reabsorption.
•Many studies and case reports (listed in this article) have found that DMSO improves renal function in patients with amyloidosis. For example, this study of 15 patients with amyloid A amyloidosis resulting from autoimmune conditions improved the kidney function in 5 out of 10 renal amyloidosis patients but could not help severe cases, while this study of two people with renal failure found both had a dramatic improvement from DMSO.
•DMSO was also found to inhibit the kidney’s Na+-K+-ATPase pump in a comparable degree to Ouabain or atrial natriuretic peptides (ANP), but did so in a manner independent from how either functioned.
Note: Ouabain or its derivatives are often used in integrative cardiology, while ANP is a naturally occurring hormone that protects both the heart and kidneys.
A rabbit study found DMSO caused an increase in filtration fraction, and at high concentrations, a decrease in renal blood flow and urine volume.
•Exposing kidney cells to 10-20% DMSO was found to increase their metabolism, while higher concentrations (which are never used in humans) was found to be toxic to the kidneys.
Autoimmune Diseases
•Many kidney autoimmune diseases result from immune deposits in the kidneys (one of which is Heymann nephritis, an experimentally induced form of nephritis where antibodies that target the kidneys are injected causing immune deposits on the glomerular walls). In a rat study of Heymann nephritis, DMSO was found to reduce protein leaking into the urine, suggesting it prevents autoimmune kidney damage. Another rat study (which was more detailed) also had similar results, as did a third rat study.
•A study of 56 DMSO treated rats (and 48 controls) with lupus nephritis found that those who received DMSO had nearly normal kidneys, whereas the controls had significant damage to their kidneys.
Kidney Stones
•A study of 6 patients with kidney stones (5 of which were confirmed by ultrasound) found IV DMSO resolved the condition in 2-3 treatments (although one patient had a complete resolution after a single infusion).
Note: I located a rat study which I believe found similar results, but I could not find the actual study to verify this.
A 1967 study fed rats a diet designed to create kidney stones, and found that after two months, 40 of the 45 water-drinking rats had developed stones in the kidney, bladder or ureter, while only 11 of the 46 DMSO group did.
Note: the author of that study later conducted another studythat strongly suggested DMSO eliminated kidney stones by improving their colloidal dispersion (zeta potential). We in turn, have had a great deal of success treating kidney stones by improving the physiologic zeta potential.
Genitourinary Disorders
In a previous article, I presented a wealth of evidence that DMSO (either consumed orally or directly administered into the bladder) with a catheter is often extremely helpful for inflammation of the bladder, particularly “interstitial cystitis” (also known as painful bladder syndrome), a challenging condition which results in very frequent, painful (and often bloody) urination.
DMSO, however can also help many other parts of the urinary tract. For example, consider this 1967 study:
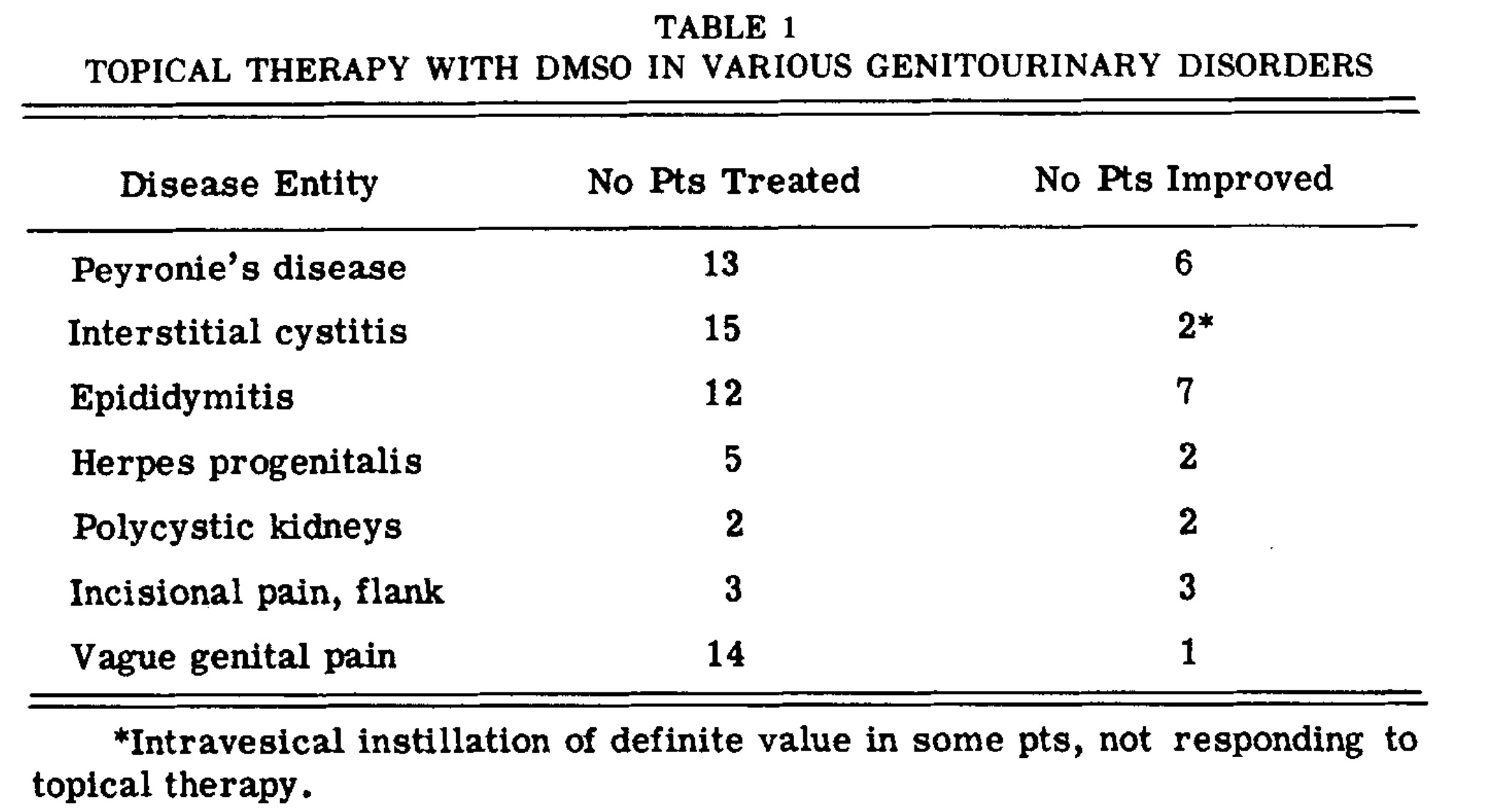
Likewise, a study (which can be viewed here) of inflammatory conditions of the urinary tract, in addition to showing significant benefit for interstitial cystitis, also found:
•Of the 12 patients with radiation cystitis (e.g., from prostate cancer therapy) 50% had a positive response to it (3 “excellent,” 2 “good” and 1 “fair”).
•Of the 35 patients with chronic prostatitis, 75% benefited significantly, with 12 having a “excellent” response, 14 a “good” response, and in 90% of cases, inflammation of the prostatic urethra improved.
Another study gave 4 men with chronic excessive (and untreatable) urination due to either chronic prostatitis, chronic cystitis, tuberculous contracted bladder and interstitial cystitis DMSO. Three of the four had an excellent response to treatment, with the one non-responder having an unclear disease process (the doctors’ best guess was that it was chronic cystitis).
•Finally, a Polish study found urethral syndrome (chronic irritation of the urethra without signs of an infection) responds to DMSO being put into the urethral tract.
There are also many anecdotal reports of DMSO being remarkably helpful for these conditions (e.g., one author shared that DMSO made it possible for men to resume sexual intercourse where previously pain or urethral blockage made it impossible).
Note: in a previous part of this series, I provided evidence that DMSO can treat Peyronie’s disease, an unfortunate contractile condition that causes a gradual curvature of the penis and significant pain during intercourse.
However, most of the anecdotal reports for DMSO’s use for the urinary tract are in regards to it helping the prostate. For example, Stanley Jacob MD (the pioneer of DMSO) would recommend DMSO for enlarged prostates that were making it difficult to urinate (which as one man shares allowed him to be able to sleep through the night), Pierre Kory recently shared a case of it curing a patient’s prostatitis, this reader found it helped prostate pain, and this reader found it helped difficulty urinating from an enlarged prostate). However, the most compelling account I heard came from this physician with extensive experience using DMSO:
Dmso is indeed marvelous. We gave 50 grams of Dmso i.v. daily for five months to a person who severed her lumbar spinal column. No organ damage noted from the Dmso and she can now drive and walk albeit slowly. Approximately forty (out of forty) patients with confirmed bacterial prostatitis have eliminated the bacteria in their prostate with a single dose of antibiotic dissolved in Dmso administrated via catheter three times a week for 4 weeks. No recurrences.
Note: Jacob also shared with an author that a physician in Texas some years earlier had reported injecting DMSO plus progesterone into enlarged prostates and that biopsies, examined under the microscope, indicated a return toward normal (which seems plausible as like DMSO, progesterone has been reported to shrink enlarged prostates).
Ovaries and Uterus
A few studies also show DMSO can help the reproductive tract:
•A rat study found that DMSO plus erythropoietin protected the ovaries from ischemia-reperfusion injuries.
•A 1975 Chilean study at a Navy hospital took 69 women who were infertile due to an obstruction in their fallopian tubes and injected a DMSO mixture into their fallopian tubes via ascendent hydrotubation (the specific mixture was 5ml of DMSO, dexamethasone, and chlorpheniramine diluted in 20 ml of distilled water). A series of 6 DMSO hydrotubations was given (every 3 days) followed by temporary breaks of varying lengths, and then an evaluation to determine if the tubes had opened. Once the tubes were opened, the patient was instructed to lead a normal sex life, and then repeat the hydrotubations if they had not gotten pregnant.
The authors reported carrying out a total of 426 DMSO hydrotubations in 69 patients, of whom 47 were available for analysis at the time the article was published. Of those 47, 27 (57.4%) subsequently became pregnant, including one who got pregnant twice (without any further assistance). Of the 27 pregnancies, 12 resulted in successful deliveries, 7 had a normal pregnancy at the time of publication, 4 patients chose to have abortions, and 3 had spontaneous abortions, and 1 had an abnormal pregnancy requiring a surgical intervention, and 0 had ectopic pregnancies (one of the risks of surgically opening the fallopian tubes). Additionally, in the 426 DMSO hydrotubations, 4 experienced discomfort and fatigue during the procedure, and 2 had psychiatric changes (in one case a sensation of anguish with difficulty breathing and in the other hypothymia and psychomotor agitation). These rare side effects (occurring in 1.5% of intubations) did not require suspending the treatment, and did not increase overtime.
Note: 25-35% of infertility is due to tubal obstructions (typically from inflammation there). The current surgical approach for opening a tubal obstruction and restoring fertility (which bears some risks) has a 10-30% success rate (figures on this vary widely, but are almost always under 50%).
•This horse study and this horse study) found that applying DMSO directly into the uterus does not harm its lining (the endometrium).
Note: there are many studies showing DMSO prefers the function and structure of tissues that get frozen (e.g., this one of a horse’s uterine lining).
•One study administered 10-30% DMSO into the uteruses of horses that could not get pregnant. It found no harm occurred to the lining of the uterus and that 18 out 27 had significant improvement to the lining of their uterus (compared to 2 out of 18 who received a saline placebo), such as a reduction of chronic inflammatory cell infiltrates and reduction of periglandular fibrosis. Additionally, there were signs their fertility improved, but the trial's design made it impossible to be sure this improvement occurred.
Note: these results suggest administering DMSO directly into the uterus could help a few challenging gynecologic conditions, but I do not know of anyone who has tried this approach.
A New Therapeutic Principle
When DMSO was discovered, Stanley Jacob quickly realized that it represented a new therapeutic principle since it made so many things which had previously seemed impossible in medicine suddenly possible—and even more remarkably, 60 years later, many of the things DMSO can address still remain a perpetual challenge for the current medical paradigm. As such, I find it remarkable that in the brief time DMSO was in widespread use and being researched worldwide, so many different uses for it that are still just as applicable today were discovered.
For example, much in the same way I recently showed how DMSO could significantly improve surgical outcomes, the data here makes good case that DMSO should be a mainstay therapy whenever someone is at risk of organ failure from being poisoned (e.g., due to a drug overdose). Likewise, the data here shows how numerous immensely challenging diseases that require a hospital or intensive care admission could be dramatically improved with DMSO.
However, while this stonewalling is immensely unfortunate, I am extremely hopeful that we will soon see a paradigm shift on this issues as:
•Much of the public (and much of the medical profession) has lost faith in the medical orthodoxy’s verdict on what does and does not work.
•Twitter (𝕏) now allows the rapid diffusion of information, making it impossible to censor the medical truths the public is craving.
•The incoming administration (particularly RFK Jr.) are strongly committed to this issue.

As such, my goal is now transitioning to trying to support this paradigm shift.
Protocols
In the final part of this article, I will discuss how DMSO can be used to treat the conditions listed throughout this article (e.g., cirrhosis, prostate enlargement, GI ulcers, ulcerative colitis), along with a few other integrative approaches we use for those conditions (e.g., for ARDS, heart attacks, gallstones, gastric bleeds, and smoke inhalation). Additionally, I will also provide a revised set of simplified instructions for the product sourcing and general use of DMSO (as I’ve received a lot of useful feedback over the last few weeks that has provided some important hints for ensuring safety).
Specific Conditions
ARDS: during COVID, we discovered the type of lung damage and respiratory distress it frequently caused (that often put patients on ventilators) responded remarkably well to exosomes, and saw numerous causes of it immediately improve from a single exosome infusion. Fortunately, DMSO is much cheaper than exosomes. Likewise, one’s survival with ARDS while on a ventilator is highly dependent upon the skill of the doctor, so it’s essential the right person is doing that (and I believe one of the reasons there were so many ventilator deaths during COVID-19 was because there weren’t enough well-trained doctors to properly supervise the ventilators in the hard-hit areas).
Cirrhosis: there are a few different schools of thought on this one. Some believe that DMSO is best consumed orally (e.g., in the successful cirrhosis study I mentioned above, they were given one teaspoonful of [presumably 100%] DMSO in one ounce of aloe vera juice two times a day for a period of six months). Alternatively, others believe you want to avoid taking DMSO orally for liver diseases since things you consume orally typically have to pass through the liver’s portal system before entering the bloodstream, and hence advise using IV or topical DMSO for cirrhosis. In practice, we find certain things work much better for the body if they bypass the portal system (e.g., we prefer topical estrogen and progesterone to ingested forms). However, I’m not actually sure if this is applicable here (e.g., oral DMSO may still bypass the portal system). Like many other conditions, it’s best to start at a low dose and gradually build up as appropriate (e.g., for cirrhosis start at 0.1 gram of DMSO per kilogram of body weight).
Gallstones: there are a lot of approaches to gallstones, but the simplest ones I’ve seen work was to take taurine (a common supplement) regularly as this aids the body in dissolving them.
Gastric or Intestinal Bleeding: there is a well-known Chinese herbal formula (Yunnan Baiyao) that is incredibly effective for stopping bleeding (in a future article I will share some of the remarkable stories we have about it). Early in my career, I had a friend who had chronic gastrointestinal bleeding (which led to them requiring iron infusions and frequently becoming deathly anemic). Knowing what Yunnan Baiyao could do, I suggested it and got my friend their life back. Since that time, I’ve researched the herb and found out it works for these types of situations.
Heart Attacks: there are a lot of approaches I have learned over the years for treating heart attacks (e.g., quite a few people have had luck with drinking Cayenne pepper solutions). Within the scope of what I’ve discussed so far here, DMSO can often help (drink it on the spot and apply it over the heart), but we’ve also seen heart attacks resolve on their own by having someone drink a properly diluted zeta aid mixture.
Note: you want to get emergency help as soon as possible here and not do anything to delay it, but we have seen these therapies immediately end heart attacks—so exactly how you’d use them would very much depend on the situation and how far the heart attack had progressed.
Kidney Stones: I strongly suspect the value of DMSO will vary depending on the type of kidney stone present (which to the best of my knowledge was never researched). Typically, we address kidney stones by focusing on zeta potential (since kidney stones are simply the result of poor zeta potential causing their components to clump together). In less severe cases, kidney stones can be treated by drinking zeta aid and deionized water. In more serious cases, IV EDTA (at a low dose) is the most effective agent we have found for dissolving them.
Prostate Enlargement: We’ve found topically applying it to the perineum often works. Dr. Jacob however found a more invasive approach to be more effective.
Dr. Jacob tried DMSO with a series of prostate massages. The pressure disappeared. I no longer had to get up during the night; I sleep until six-thirty or seven-thirty in the morning without having to go to the lavatory I have no discomfort whatever. That was sixteen or seventeen months ago. I still get treated occasionally But that condition is under control.
Prostatitis: Patients with prostatitis often respond to other routes of DMSO. However, in the study I cited with the highest success rate, this was the approach they used (which was essentially an attempt to get DMSO more directly to the prostate).
Here, a Robinson catheter of 14-16 F was passed gently to the level of the membranous urethra, and the medication was slowly instilled directly into the prostatic urethra and then into the bladder. In some cases the panendoscope was passed under direct vision to the level of the membranous urethra, and the medication instilled through the panendoscope directly into the prostatic fossa. In occasional patients with severe symptoms, this appeared to afford the greatest relief, although admittedly part of the good results could have been psychologic in nature.
Smoke Inhalation: While I do not have that much experience nebulizing DMSO for it, we have found that nebulized glutathione (discussed further here) is extremely helpful for individuals who have been injured by wildfire smoke.
Gastroinestinal disorders (e.g., ulcerative colitis or duodenal ulcers): In the studies I reference, the oral DMSO dose was 500mg of DMSO 4 times a day (which is approximately half a teaspoon of 100% DMSO four times a day).
Genitourinary disorders: in the studies I referenced, these were either treated with intravesical administrations or topical administration (of 50-100% DMSO) over the problem areas.
Sourcing DMSO:
There are a lot of options when purchasing DMSO. Of them, I’ve longed believe these are the three best brands (which I’ve included Amazon links to purchase them):
•Jacob Lab (e.g., this gel or this liquid)—which is 99.98% pure.
•Nature’s Gift (e.g., this gel or this liquid)—which is 99.9% pure.
•The DMSO Store (e.g., this gel or this liquid)—which is 99.995% pure.
Note: unless you feel confident you can dilute them correctly, get the 70% ones, since that concentration typically works for people.
When buying liquid DMSO, I believe it should always be sold in a glass container unless the plastic container is DMSO resistant (which many are not—hence why I only recommended buying glass bottles) and likewise have a DMSO resistant cap. If you buy gel, it’s fine if it’s sold in plastic.
Note: many people have used liquid DMSO from plastic containers without issue, but I have personally always avoided doing so because glass DMSO has always been affordable and easily available.
The unexpected problem I ran into was that many of the people who ordered glass DMSO from the links I recommended then informed me they had been shipped in plastic (which is likely either because those parties were resellers or because everyone ran out of glass bottles and the DMSO market is currently trying to rebuild that inventory).
Of the currently existing options, I believe the best choice is to either:
•Buy DMSO directly from the DMSO store (DMSOstore.com).
Note: the website DMSO.store is for a completely different company.
•Buy it directly from Jacob lab (which readers have informed me is also shipping DMSO in plastic they claim is DMSO resistant—which it likely is since Stanley Jacob worked with them for years).
DMSO dosing:
One of the things that’s very challenging about using DMSO is that there is a significant amount of variation in what each individual will best respond to. Because of this, in the first and second parts of this series, I attempted to provide a very detailed explanation that could try to account for each possibility which may have been too complicated (but I would still advising reading).
So the major consideration is how strong of a dose you want to use. This is because if you use too high a dose, you risk the chance of having a bad reaction, which will make you not want to use DMSO anymore, whereas if you use too low of a dose, the effect will be much less than desired. In turn, I’ve had many people here who:
•Applied 100% DMSO topically and had trouble believing anyone couldn’t tolerate that.
•Applied 70% DMSO topically, had a bit of irritation but thought it was manageable.
•Applies 30% topically and felt it was too strong.
Similarly with oral dosing, I’ve had people who:
•Thought 1 teaspoon was decent but quickly took more for a greater effect.
•Found a few drops was the optimal dose for them (and greatly benefitted) whereas 1 teaspoon while initially good, ended up feeling like it was too much for them.
Because of this, you essentially have two options, and have to decide which is right for you:
•Be patient and start with a low dose you build up.
•Start a strong dose and agree not to hold it against me or DMSO if you don’t tolerate it.
In the previous articles, I advocated for the former. Still, many understandably started with a high dose as they did not want to wait for the results, a few of whom then shared they’d had a skin reaction that made them hesitant to continue using DMSO.
Similarly, when using DMSO, there are two common routes of application, orally and topically. Orally, it is much stronger, but likewise, the GI tract is more sensitive to higher concentrations of DMSO. For this reason, I typically suggest starting with topical DMSO before doing oral DMSO. Likewise, there is a very small risk (1 in 1-2000) of an allergic reaction, so it’s generally advised to begin by patch testing DMSO on the skin before taking it orally.
So, What is Patch Testing?
Patch testing is a method used to determine how the application reacts to a product. It's a smart way to test a small area first before applying the product to larger areas, which helps to identify any adverse reactions.
How to Patch Test:
•Select a Small Area: Choose a discreet spot.
•Apply a Tiny Amount: Use a small quantity of the product.
•Wait and Observe: Leave it on for 24 hours unless you notice irritation sooner.
•Proceed if All’s Good: If there’s no reaction, feel confident to use the product as intended!
*If in contact with the skin: Some experience itching and tingling sensations, which are normal. If there’s any redness or swelling, wash the area immediately and discontinue use.
That said for general DMSO use (without going into all the nuances and additional details), I advise the following:
Start with 30-50% DMSO and see how you tolerate it.
If you have no issue, raise it to 70%.
Only raise it past 70% if you are certain you are one of those people who is fine with 100% or you are using it for a specific application that can justify a higher concentration (e.g., a collagen contracture, a scar, an internal adhesion or an acute stroke).
Until you are comfortable with topical applications, don’t do oral applications, and only if you think you need them.
For oral dosing, start with a teaspoon of 70% or 100% DMSO mixed into a glass of water (you may also want juice or milk to eliminate DMSO’s taste).
If you have issues with that, lower the dose to half a teaspoon and then to a quarter teaspoon.
Otherwise, stay at a teaspoon for at least three days, and then if you think you need a stronger effect, go to 2 teaspoons.
More than 3 teaspoons in a glass of water is excessive, and at that point, you are better off dividing the dose throughout the day.
With both topical and oral DMSO, people generally find that as time goes on, their tolerance to it improves. Conversely, if it’s used too frequently, a tolerance can develop, so it’s generally advised to not have it 1-2 days a week.
Note: more detailed instructions on oral (and IV) DMSO use can be found here, while more detailed instructions on topical uses can be found here.
Regarding the concentrations used, I generally advise buying 70% DMSO because people rarely react to it (e.g., the DMSO felt it was the concentration that had the best balance between safety and efficacy). It doesn’t require any significant calculations to dose appropriately (e.g., you can apply it topically as it is, or mix it with equal parts of purified water to get it to roughly 35%). However, you can also do all of that with 100% DMSO (e.g., dilute it to roughly 50% rather than 35% by mixing it with equal parts of purified water or to roughly 33% by mixing it with two parts of purified water). Finally, certain parts of the body, particularly the face, tend to be more sensitive to higher concentrations of DMSO, so you should start at lower strengths in those areas.
Additionally, the one tricky thing about dosing DMSO is that it weighs slightly more than water (1ml of DMSO is 1.1004 grams). Since there is a fairly wide range of tolerability to DMSO, I’ve bypassed that issue here by treating it as having the same density as water and suggesting a slightly lower oral dose.
Note: when DMSO is taken by mouth, the total concentration should always be kept to 20% or less, and ideally, it should be taken slowly after eating a meal.
When applying DMSO topically, there are two options. The first is to use a liquid that you directly apply (e.g., I like to use natural hair paintbrushes to dab it on, but sometimes when needed I just dip my finger in it and then rub it onto the target area). The second is to use a gel which is rubbed into the skin.
When applying DMSO to the body, it is important to clean the area it will be applied to beforehand, and to ensure DMSO dries before putting anything in contact with it. This is because DMSO will pulling things on the surface of the skin into the body, and if a toxic chemical is on the skin, it hence will be dragged into the body. This is very rare, but there are known instances of this happening and harming the individual.
I personally prefer the liquids because it’s easier to control the total dose with them, more gets into the body, and liquid DMSO tends to be less irritating. That said, gels hold the advantage of continually releasing DMSO into the body over a prolonged period and are much easier to apply. Because of this, whichever one you use is largely a question of personal preference.
In most cases, if an area bothers you, you are better off applying DMSO to that area (provided there is no open wound), but if the issue feels systemic, you may also need to take oral DMSO.
Note: for many of the conditions described here (e.g., interstitial cystitis) even though DMSO was primarily given through catheters that emptied it into the bladder, many clinicians have found it works just as effectively when taken orally (and did not subject the patient who were already so irritated they could not tolerate a catheter going in).
Conclusion
I hope you have appreciated this series so far. I have put a lot of work into it, and based on all the reports I’ve been coming across (from both readers and colleagues), it seems to be doing much more for the world than I ever expected it could. Fortunately (for me) we’re at last over halfway through it.
For those of you who are wondering, the remaining parts of this series will be:
•How DMSO can be used for challenging diseases of the skin and the related issues like hairloss.
•How DMSO transforms the treatment of cancer and infectious diseases.
•How DMSO can be mixed with a variety of other therapeutics.
•A summary of all the reader DMSO feedback I’ve received.
•A summary of this entire series.
I sincerely thank each of you for helping support me write this, helping to share this information with those who can most benefit from it, and for helping to create the new political climate we are walking into which will at last make it possible to have a healthy medical system!















There was an editing error while writing this which caused the content in the section "kidney function" to get deleted. It has been restored.
OK, I hesitate to share this, but here goes.
Because of Midwestern Doctor's articles, I've been experimenting with DMSO for several months now. I have a spondylolisthesis in my low back where L4 has shifted 20% forward over L5 from an injury five years ago. This has caused severe stenosis and basically the spinal nerves from that area are severely impinged, causing a spectrum of pain (from intense aching to a searing sensation of flesh tearing away from bone) throughout my hips and sacral area as well as persistent sciatica in one, or sometimes both, legs.
I've been using DMSO (from DMSOstore.com, 99.995 pure, undiluted) topically throughout my sacral area, then also on my hips, then lately on my calves (that would ache after exercise). The DMSO reduced my perceptions of pain considerably. I carefully reread all the articles about dosing and non-toxicity and thought maybe if I use more, I can eliminate the pain entirely.
I increased the frequency (to every four hours, up from once or twice a day) and the volume (from roughly one tablespoon to 2-4 tablespoons applied topically). I could not eliminate the pain completely, but after a few days, there was this amazing side effect.
A minute or two after applying the DMSO I had this unanticipated erection, I mean a raging hard-on. Mind blowing. I'm a 75-year old male with no ED problems, but having so much pelvic pain, I haven't had, nor thought about sex for a long time. I wasn't having any stimulating thoughts, I was just going through my self-medication routine and... boing!
Ever since then (last week), every time I apply an extra large dose, I experience this effect. I suspect that DMSO's enhancement of blood flow might be at work here. Plus, all the nerves that go to my genitals are compromised by impingement, so maybe DMSO helped them out. Also, I've noted a psychological effect, more calm and serene. I can attribute that to "I feel better not being in so much pain," though there may be a physiological component to the emotional uplift.